Master your cycle, maximize your chances, and take control of your conception journey.
When is your fertile window?
Your fertile window is the 5 days before ovulation plus ovulation day—a 6-day period when conception is possible. This window exists because sperm can survive up to 5 days in fertile cervical mucus, while the egg lives for only 12-24 hours after ovulation. The best time to conceive naturally is intercourse 1-2 days before ovulation, when conception probability peaks at 27-31%.
How long is the fertile window? The fertile window is typically a 6‑day period. Can you get pregnant outside the fertile window? It is extremely unlikely because conception requires both viable sperm and a viable egg to be present at the same time, which almost always happens only within these 6 days each cycle.
In this article
When is your fertile window? The 6-day conception period explained
Your fertile window definition: The 5 days before ovulation plus the day of ovulation itself—a total of 6 days when conception is possible.
This 6-day window is determined by two biological factors:
Sperm survival: Sperm can live up to 5 days in fertile cervical mucus, waiting for the egg to be released
Egg viability: The egg lives for only 12-24 hours after ovulation
Understanding your fertile window is essential for conception timing. Research shows that intercourse during this 6-day period gives sperm time to reach the egg when it's released, making timing the single most critical factor in achieving pregnancy.
Source: American Society for Reproductive Medicine (ASRM). (2022). "Optimizing Natural Fertility: A Committee Opinion." www.asrm.org
How to calculate your fertile window with irregular cycles
The biggest misconception in TTC (trying to conceive): that every woman ovulates on day 14 of a 28-day cycle.
The reality: Only about 30% of women have their fertile window entirely within days 10-17. The rest ovulate earlier or later depending on their unique cycle length.
Your ovulation timing depends on:
Cycle length: Women with 25-day cycles may ovulate on day 11; women with 35-day cycles may ovulate on day 21
Stress and illness: Can delay ovulation by several days
Lifestyle factors: Exercise, weight changes, and sleep patterns affect hormone balance
The hormonal signals behind your fertile window
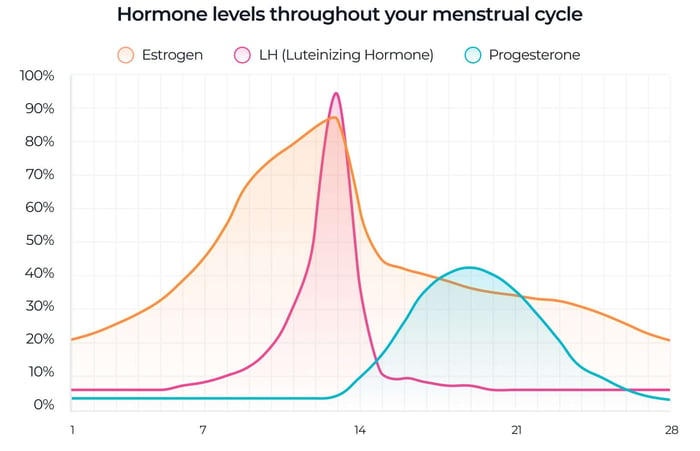
Your menstrual cycle operates on precise hormonal timing:
Follicular phase (days 1-14): Estrogen rises as follicles develop, thickening the uterine lining and producing fertile cervical mucus
LH surge (24-36 hours before ovulation): Luteinizing hormone spikes, triggering the release of the egg
Ovulation (peak fertility): The egg is released and lives for 12-24 hours
Luteal phase (post-ovulation): Progesterone dominates, closing the fertile window
Source: Mu Q, Fehring RJ. (2023). "Hormonal Fertility Monitoring Systems for Ovulation Detection." Medicina (Kaunas). DOI: 10.3390/medicina59020400
Tracking the LH surge is the most reliable way to pinpoint your fertile window. Modern ovulation predictor kits (OPKs) detect this surge 24-36 hours before ovulation, giving you advance notice of your peak fertility days.
⏰ Timeline: From LH Surge to Conception Window
Day 0 (Morning)
LH surge begins — Your ovulation test turns positive (T/C ratio ≥ 1:1). This is your signal to start having intercourse.
12-24 hours later
Peak LH levels — Hormone reaches maximum concentration. Continue intercourse every other day.
24-36 hours later
Ovulation occurs — This is your peak fertility window. The egg typically survives for 12–24 hours after release.
Within 24 hours of ovulation
Fertilization window — Sperm meets egg in the fallopian tube. This must happen within 12-24 hours of ovulation.
6-12 days later
Implantation — Fertilized egg implants in uterine lining. You can test for pregnancy 10-14 days after ovulation.
Key takeaway: The positive ovulation test gives you a 24-36 hour advance warning before your egg is released—perfect timing to maximize conception chances.
Ready to pinpoint your fertile window?
Pregmate ovulation test strips are described in the source article as detecting the LH surge with 99% accuracy, helping users identify peak fertility days.
How to recognize natural fertility signs
Your body provides physical signals that your fertile window is opening:
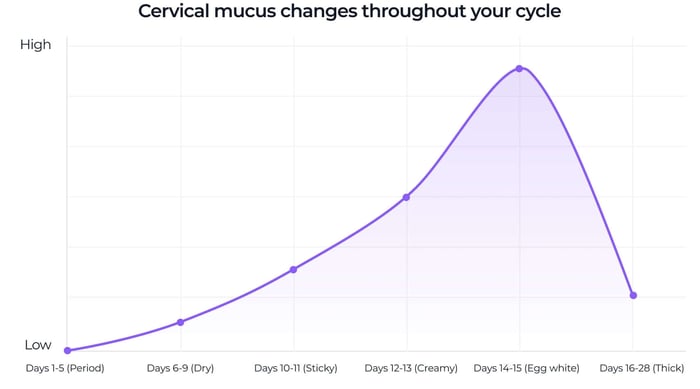
Cervical mucus changes
Early cycle: Dry or sticky mucus (low fertility)
Approaching ovulation: Clear, stretchy, slippery mucus resembling raw egg whites (high fertility)
After ovulation: Mucus becomes thick and cloudy (fertile window closed)
Why it matters: Fertile cervical mucus nourishes and transports sperm, extending their lifespan to 5 days. Without it, sperm survive only 1-2 days.
Other fertility signs
Increased libido: Many women notice a natural boost in sex drive during their fertile window
Mittelschmerz: Light cramping or twinges on one side of the abdomen at ovulation
Basal body temperature (BBT): Rises 0.5-1°F after ovulation, confirming the fertile window has closed
Pro tip: Combine physical signs with ovulation tests for maximum accuracy. Physical signs warn you the window is opening; OPKs pinpoint the exact peak.
Source: Bigelow JL, et al. (2004). "Mucus observations in the fertile window: a better predictor of conception than timing of intercourse." Human Reproduction. DOI: 10.1093/humrep/deh173
Best time to have sex during your fertile window for natural conception
Remember: The test line must be as dark as or darker than the control line to be truly positive. A faint line means keep testing!
Modern fertility tracking combines body awareness with technology:
Ovulation predictor kits (OPKs)
How they work: Detect the LH surge 24-36 hours before ovulation
Best for: Women who want precise timing and actionable data
Pregmate ovulation test strips offer clinical-grade accuracy at $0.30-0.50 per test—ideal for daily or twice-daily tracking.
Fertility tracking apps
How they work: Combine cycle history, BBT, cervical mucus data, and OPK results to predict fertile days
Best for: Women who want to see patterns over multiple cycles
The Pregmate app syncs with Pregmate ovulation tests to automatically track your LH trends, send testing reminders based on your cycle, and visualize your fertile window in real-time.
Basal body temperature (BBT) tracking
How it works: Confirms ovulation occurred (temperature rises 0.5-1°F after)
Best for: Confirming patterns, not predicting in real-time
Using Pregmate ovulation tests to pinpoint your exact fertile window
While understanding the 6-day fertile window is essential, knowing exactly when those 6 days occur in your cycle is what actually gets you pregnant. This is where Pregmate ovulation test strips can help you detect your LH surge.
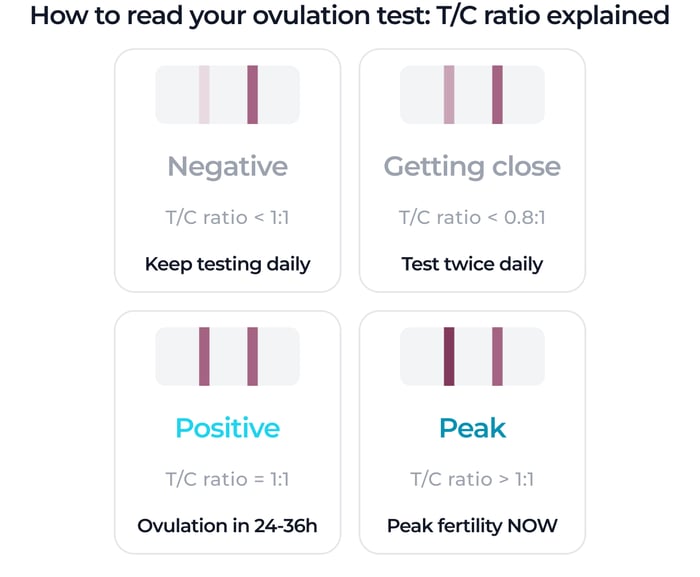
What a positive OPK actually looks like: the T/C ratio explained
Unlike pregnancy tests where "any line = positive," ovulation tests work differently. Here's what you're actually looking for:
Test line (T) = LH detection line (the one that changes)
Control line (C) = Reference line (always appears)
T/C ratio = Darkness of test line compared to control line
Reading your result:
T/C < 0.8 (T lighter than C): Negative — LH surge hasn't started yet
T/C ≥ 1.0 (T as dark as or darker than C): Positive — LH surge detected, ovulation likely in 24-36 hours
T/C > 1.2 (T noticeably darker than C): Peak surge — ovulation imminent
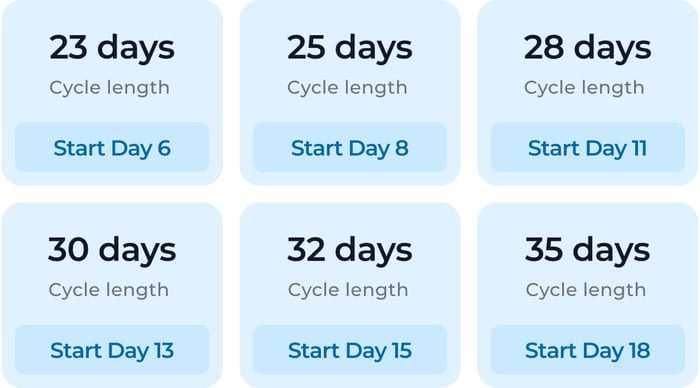
When to start testing based on your cycle length
Don't waste tests or miss your window. Here's when to start:
| Cycle length | Start testing on | Expected positive day |
|---|---|---|
| 23-25 days | Day 6-8 | Day 9-11 |
| 26-28 days | Day 9-11 | Day 12-14 |
| 29-32 days | Day 12-15 | Day 15-18 |
| 33-35 days | Day 16-18 | Day 19-21 |
| Irregular or PCOS | Day 6-8 | Varies, test daily |
Formula: Cycle length - 17 days = Start testing day. Example: 30-day cycle → Start Day 13.
Real LH surge patterns: what to expect
Not everyone's LH surge looks the same. Here are the 3 most common patterns:
📈 Pattern 1: Gradual Rise (40% of women)
What it looks like: LH slowly increases over 2-3 days before spiking. You'll see T/C go from 0.3 → 0.6 → 0.9 → 1.2 → 0.7.
Action: Once T/C reaches 0.8-0.9, start having intercourse every day. Don't wait for the "perfect" positive.
⚡ Pattern 2: Sharp Peak (50% of women)
What it looks like: LH jumps from barely visible to positive in 12-24 hours. T/C goes 0.2 → 0.3 → 1.1 in one day.
Action: Test twice daily (morning + late afternoon) to catch the surge. Once positive, have intercourse same day + next 2 days.
🔄 Pattern 3: Double Peak (10% of women)
What it looks like: LH surges, drops, then surges again 1-2 days later. The second peak triggers ovulation.
Action: If your positive line fades then darkens again, keep testing. The second peak is your true ovulation signal.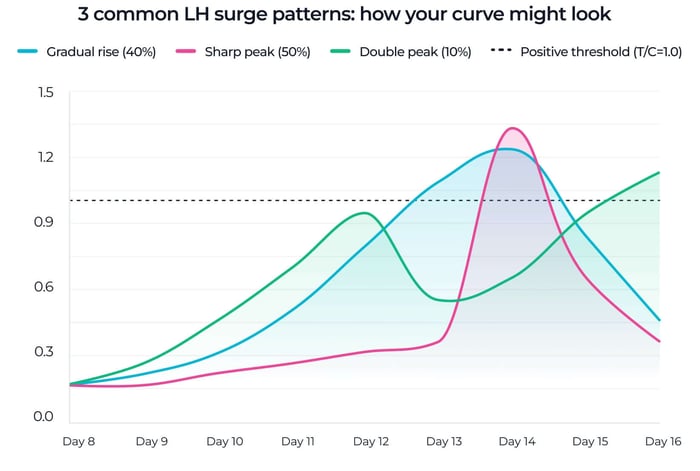
Reference: Based on LH variability data from Mu & Fehring 2023
Real-life scenarios: putting it all together
Scenario 1: Regular 28-day cycle
Start testing: Day 11
Expected positive: Days 12-14
Fertile window: Days 9-14 (approximately)
Best intercourse timing: As soon as T/C ≥ 0.8, have intercourse that day + next 2 days
Scenario 2: Irregular cycles (25-35 days)
Start testing: Day 8 (earliest possible ovulation)
Testing frequency: Once daily until T/C reaches 0.5, then twice daily
Expected positive: Could be anywhere from Day 11-21
Best intercourse timing: Start every-other-day intercourse from Day 8, switch to daily once T/C ≥ 0.8
Scenario 3: PCOS or very long cycles (40+ days)
Start testing: Day 10-12
Testing frequency: Daily until LH starts rising, then twice daily
Expected positive: May take 2-3 weeks of testing
Challenge: False LH "mini-surges" common with PCOS — look for T/C ≥ 1.0 sustained for 24+ hours
Ready to pinpoint your fertile window?
Pregmate ovulation tests detect your LH surge 24-36 hours before ovulation—giving you advance warning of your most fertile days. Available in 25, 50, and 100-count packs for any cycle length. Clinical-grade accuracy at just $0.30-0.50 per test.
Fertile window timing: when to have intercourse for pregnancy
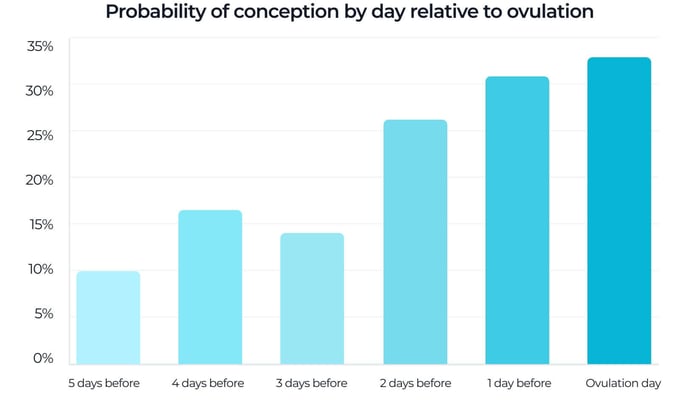
Not all 6 days are equally fertile. Research identifies the highest conception probability:
| Day relative to ovulation | Approximate probability of conception |
|---|---|
| 5 days before | ~10% |
| 4 days before | ~16% |
| 3 days before | ~14% |
| 2 days before | ~27% |
| 1 day before | ~31% |
| Day of ovulation | ~33% |
Key takeaway: The 2 days before ovulation and ovulation day itself account for nearly all conceptions. Having intercourse before the egg is released is more effective than waiting until ovulation day.
How often to have intercourse during the fertile window
Every other day is optimal. This frequency:
Maintains high sperm count and quality (abstinence > 5 days reduces quality)
Covers the fertile window without creating stress
Balances biological timing with relationship enjoyment
Alternative approach: If you pinpoint ovulation precisely with OPKs, aim for the day before ovulation, ovulation day, and the day after.
Factors affecting your ovulation timing and fertile window
Ovulation timing isn't fixed—it responds to your body's overall health and environment:
Stress and sleep
Chronic stress: Elevates cortisol, which can delay or suppress ovulation
Poor sleep: Disrupts melatonin and reproductive hormone balance
Weight and exercise
Underweight (BMI < 18.5): May prevent ovulation altogether
Overweight (BMI > 25): Can cause irregular ovulation and longer cycles
Excessive exercise: High-intensity training can suppress the menstrual cycle
Nutrition and supplements
Folate: Essential for neural tube development—start prenatal vitamins 3 months before TTC
Vitamin D: Deficiency linked to irregular cycles
Omega-3 fatty acids: Support hormone production and egg quality
Good lifestyle habits make your cycles more predictable, which makes fertile window tracking more reliable.
How to find your fertile window with PCOS or irregular periods
Irregular cycles make prediction harder—but not impossible. Here's how to adapt:
Start testing early: Begin OPK testing on day 6 of your cycle and continue daily until you detect the surge
Test twice daily: If cycles are very unpredictable, test at 10 AM and 6 PM to avoid missing short LH surges
Track cervical mucus: Physical signs provide advance warning even when ovulation day varies
Use an app to identify patterns: Over 3-6 months, even irregular cycles often reveal a pattern (e.g., ovulation occurs 14 days before period, even if cycle length varies)
When to see a doctor
If cycles vary by more than 7-10 days regularly, or if you never detect ovulation after 3 cycles of testing, consult a reproductive endocrinologist.
Common myths about the fertile window
❌ Myth 1: You can only get pregnant on ovulation day
✅ Truth: Sperm survival (up to 5 days) makes the days before ovulation equally—or even more—fertile. In fact, conception is most likely when intercourse occurs 1-2 days before ovulation.
❌ Myth 2: All women have a 6-day fertile window
✅ Truth: While 6 days is the biological maximum (5 days sperm survival + 1 day egg viability), individual variation in sperm quality, cervical mucus, and cycle regularity can shorten the effective window.
❌ Myth 3: Everyone ovulates mid-cycle
✅ Truth: Only 30% of women have fertile windows entirely within days 10-17. Cycle length, stress, and health shift ovulation timing significantly.
❌ Myth 4: Having sex every day increases chances
✅ Truth: Daily ejaculation can reduce sperm count. Every-other-day timing during the fertile window maintains optimal sperm quality while still covering peak fertility days.
The emotional side of fertile window tracking
Fertility awareness empowers couples with knowledge—but it can also create stress if approached rigidly.
Common emotional challenges
Performance pressure: Feeling like intercourse must happen "on schedule" can reduce spontaneity and enjoyment
Cycle disappointment: When the fertile window passes without conception, some couples feel like they "failed"
Testing fatigue: Daily OPK testing can feel like a constant reminder of TTC stress
How to stay balanced
Remember the odds: Even perfectly timed intercourse results in only 20-30% conception probability per cycle
Communicate openly: Discuss tracking with your partner and approach it as teamwork
Take breaks: If tracking becomes overwhelming, it's okay to skip a cycle and focus on stress reduction
Fertile window tracking is a guide, not a guarantee. Approach it with patience, realistic expectations, and kindness toward yourself.
Track your fertile window with precision
The free Pregmate app includes an OPK scanner that measures your T/C ratio objectively and maps your LH curve—so you know exactly when your fertile window opens and closes each cycle. Get personalized testing reminders based on your cycle length.
FAQ: your fertile window questions answered
- How long is the fertile window?
- About 6 days in total: the 5 days before ovulation plus the day of ovulation itself. Peak fertility happens in the final 2-3 days of that range.
- When should I have intercourse for the best chance of pregnancy?
- The strongest days are usually the 2 days before ovulation and ovulation day. Many couples aim for every-other-day intercourse during this time.
- What if I do not notice ovulation signs?
- Use ovulation predictor kits to supplement physical signs. They can detect the LH surge even if cervical mucus changes are not obvious.
- Can fertile window tracking be used to prevent pregnancy?
- Fertility awareness methods can reduce pregnancy risk when used carefully, but they are generally less reliable than medical contraception.
- When should I see a doctor?
- If you have been trying for 12 months without success, or for 6 months if you are over 35, seek medical evaluation sooner. Earlier review is also sensible with PCOS, very irregular cycles, or known fertility concerns.
- What is the difference between ovulation and the fertile window?
- Ovulation is the single event when the egg is released. The fertile window is the surrounding 6-day period when sperm can survive long enough to fertilize that egg.
Take control of your conception timing
Understanding the fertile window turns conception from guesswork into strategy. By focusing on the 5 days before ovulation and ovulation day, and especially the 2 days before ovulation, you improve your odds of timing intercourse effectively.
Ovulation tests, fertility apps, and cervical mucus tracking can work together to identify your personal fertile days, even if your cycles are irregular.
Medical disclaimer
This article is for informational purposes only and does not constitute medical advice. Fertile-window tracking and ovulation prediction can support conception timing, but they should not replace consultation with a qualified healthcare provider.
If you have been trying to conceive for 12 months without success, or for 6 months if you are over age 35, or if you have concerns about irregular cycles or fertility, consult a reproductive endocrinologist or OB-GYN.
Sources
Wilcox, A.J., Weinberg, C.R., & Baird, D.D. (1995). "Timing of Sexual Intercourse in Relation to Ovulation — Effects on the Probability of Conception, Survival of the Pregnancy, and Sex of the Baby." New England Journal of Medicine, 333(23), 1517-1521. https://doi.org/10.1056/NEJM199512073332301
Bigelow, J.L., Dunson, D.B., Stanford, J.B., Ecochard, R., Gnoth, C., & Colombo, B. (2004). "Mucus observations in the fertile window: a better predictor of conception than timing of intercourse." Human Reproduction, 19(4), 889-892. https://doi.org/10.1093/humrep/deh173
American Society for Reproductive Medicine (ASRM). (2022). "Optimizing Natural Fertility: A Committee Opinion." Fertility and Sterility, 117(3), 533-546. https://www.asrm.org/
Colombo, B., & Masarotto, G. (2000). "Daily fecundability: first results from a new data base." Demographic Research, 3, Article 5. https://www.demographic-research.org/volumes/vol3/5/
Stanford, J.B., White, G.L., & Hatasaka, H. (2002). "Timing intercourse to achieve pregnancy: current evidence." Obstetrics & Gynecology, 100(6), 1333-1341. https://doi.org/10.1016/s0029-7844(02)02382-7
Mu, Q., & Fehring, R.J. (2023). "A Comparison of Two Hormonal Fertility Monitoring Systems for Ovulation Detection: A Pilot Study." Medicina (Kaunas), 59(2), 400. https://doi.org/10.3390/medicina59020400
Gibbons, T., Reavey, J., Georgiou, E.X., & Becker, C.M. (2023). "Timed intercourse for couples trying to conceive." Cochrane Database of Systematic Reviews, 9, CD011345. https://doi.org/10.1002/14651858.CD011345.pub3
Levitas, E., Lunenfeld, E., Weisz, N., Friger, M., & Potashnik, G. (2005). "Relationship between the duration of sexual abstinence and semen quality: analysis of 9,489 semen samples." Fertility and Sterility, 83(6), 1680-1686. https://doi.org/10.1016/j.fertnstert.2004.12.045