What actually works: treatments, timelines, and realistic expectations backed by 2023-2026 research.
Key takeaways
- 77% of women with PCOS do become mothers - pregnancy is possible, but it may take longer.
- First-line treatment: lifestyle changes - 5-10% weight loss can restore ovulation in many women with overweight or obesity.
- Letrozole outperforms clomiphene in trials - about 40-42% pregnancy rates vs. roughly 30% with clomiphene citrate.
- Supplements have limited evidence - myo-inositol is not recommended specifically for fertility by international guidelines.
- Age matters more than PCOS status - seek help after 6 months if over 35, after 12 months if under 35.
- Track ovulation carefully - irregular cycles make timing crucial, so use OPKs plus apps when needed.
- Pregnancy risks are higher, but manageable - with proper prenatal care and monitoring, many women with PCOS have healthy pregnancies.
Important note
This article provides educational information only and should not replace professional medical advice. PCOS is a complex medical condition requiring individualized diagnosis and treatment by qualified healthcare providers. Always consult with a reproductive endocrinologist or OB-GYN before starting any treatment, supplement, or lifestyle modification for fertility.
In this article
While PCOS is a leading cause of infertility, most women with PCOS can achieve pregnancy. Research shows that approximately 77% of women with PCOS eventually become mothers, though conception may take longer than for women without PCOS. Treatment success rates vary based on age, BMI, and individual response.
Understanding PCOS and fertility: what the research shows
Polycystic ovary syndrome (PCOS) affects 5-15% of women of reproductive age and is characterized by irregular ovulation, elevated androgens, and often insulin resistance.
Can you get pregnant with PCOS?
Yes. A longitudinal study following women for 25 years found that women with PCOS had an average of 1.7 births, compared to 1.9 in women without PCOS. While about 23% of women with PCOS did not have children during the study period (compared to 18% without PCOS), the vast majority, 77% — became mothers.
PCOS pregnancy outcomes: 25-year longitudinal study
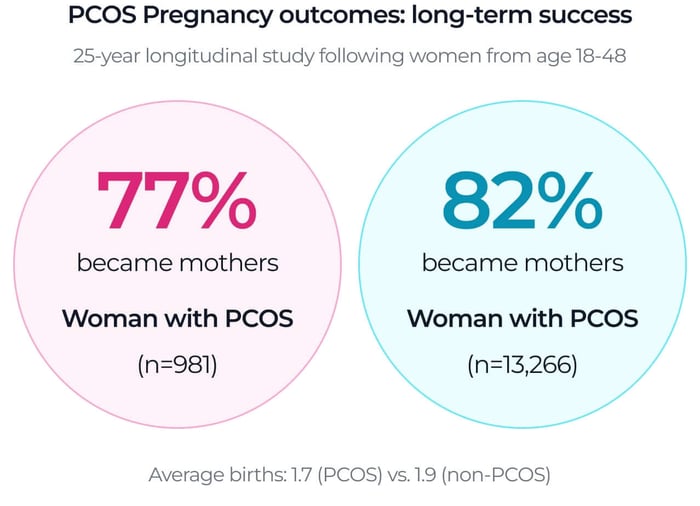
Source: Forslund et al., 2024. "Fertility and age at childbirth in polycystic ovary syndrome." American Journal of Obstetrics & Gynecology
Is it hard to get pregnant with PCOS?
It can be more challenging, but not impossible. Key factors affecting difficulty include:
Ovulation frequency: Many women with PCOS ovulate irregularly or not at all (called anovulation—when your ovaries don't release an egg)
Age: Women with PCOS tend to start fertility treatment about 3 years younger on average, but age remains the most critical factor for treatment success
BMI: Higher BMI is associated with lower ovulation rates and pregnancy success
Insulin resistance: Present in many women with PCOS, affects hormone balance and ovulation
Lifestyle modifications: the first-line approach
International guidelines recommend lifestyle modification as the first-line treatment for women with PCOS and overweight or obesity.
Weight loss (if overweight)
A 2023 randomized controlled trial found that a comprehensive lifestyle intervention (combining diet, exercise, and cognitive behavioral therapy) resulted in a 39.8% live birth rate in women with PCOS and BMI ≥25, similar to the 38.3% rate in the control group. The key finding: even modest weight loss (5-10% of body weight) can improve ovulation and fertility outcomes.
What this means
Lifestyle intervention study: live birth rates in women with PCOS
Source: Dietz de Loos et al., 2023. "Pregnancy Outcomes in Women with PCOS: Follow-Up Study of a Randomized Controlled Three-Component Lifestyle Intervention." Journal of Clinical Medicine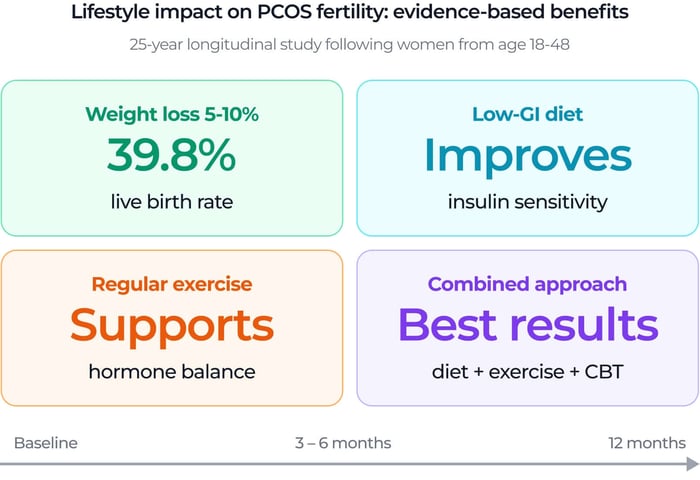
Source: Dietz de Loos et al., 2023. Pregnancy Outcomes in Women with PCOS.
Diet for PCOS fertility
While no single "PCOS diet" has been proven superior, evidence supports:
Low glycemic index foods: whole grains, legumes, and non-starchy vegetables.
Anti-inflammatory foods: omega-3 rich fish, nuts, and olive oil.
Adequate protein: Helps with satiety and blood sugar control
Limited processed foods and added sugars: Reduces insulin spikes
Note: Personalized nutrition counseling with a registered dietitian is recommended, as individual responses vary.
Start this week
1. Calculate your BMI: Weight (lbs) ÷ height (inches)² × 703. If over 25, a 5-10% weight loss can help.2. Pick one change: Don't overhaul everything. Start with one: swap white bread for whole grain, add fish twice a week, or cut sugary drinks.
3. Track your cycle: Start now, even if irregular. Use an app or paper calendar to spot patterns.
4. Find your people: Join a PCOS support group (online or local) to share what actually works.
Medical treatments: what works
Ovulation induction medications
Letrozole (recommended first-line)
A study found that women with PCOS treated with letrozole had a 41.7% pregnancy rate, compared to 32% with clomiphene citrate. Letrozole patients also required fewer cycles to achieve pregnancy (2 cycles vs. 3 cycles).
Clomiphene citrate (alternative option)
Still effective with a 32% pregnancy rate, though generally considered second-line after letrozole.
Metformin
Primarily used to improve insulin sensitivity. It may be combined with ovulation induction but is not typically used alone for fertility.
In vitro fertilization (IVF):
For women who don't respond to ovulation induction or have other fertility factors, IVF may be recommended. A 2020 study of 7,678 women found that those with PCOS actually had higher pregnancy rates with IVF compared to women with other infertility diagnoses. This is because PCOS patients often respond well to ovarian stimulation and produce good numbers of eggs.
However, PCOS patients also faced increased risks of miscarriage and preterm delivery, which is why close monitoring during pregnancy is essential.
Source: Forslund et al., 2024 — Importance of early PCOS diagnosis
Track ovulation with PCOS cycles
PCOS cycles are unpredictable, so frequent testing matters. Pregmate ovulation tests offer affordable, accurate LH tracking for women who need to test daily or twice daily.
Supplements and vitamins: what does the evidence say?
A comprehensive systematic review used for the International PCOS Guidelines found that evidence for most supplements improving fertility is currently limited or inconclusive.
The straight answer
Many women with PCOS take supplements hoping to boost fertility. The research shows supplements may help with insulin and metabolic health, but they do not replace proven medical treatments like letrozole.
Think of supplements as supporting players, not the star quarterback. Use them alongside, not instead of, evidence-based treatments. Always discuss with your doctor before starting anything new.
| Supplement | Evidence Quality | Typical Dose | Verdict |
|---|---|---|---|
| Myo-inositol | ⚠️ Limited/Inconclusive | 2-4g daily | Not recommended specifically for fertility by 2023 guidelines |
| Vitamin D | Test and supplement if deficient | Varies | Get tested; supplement under supervision if low |
| Omega-3 | May help metabolic markers | 1-3g EPA + DHA | May improve insulin and inflammation markers |
| NAC | May help insulin resistance | 600mg 2-3x daily | Limited fertility evidence |
Source: Fitz et al., 2024. Inositol for PCOS: systematic review and meta-analysis.
Myo-inositol
What it is: a sugar molecule that helps with insulin signaling.
The research: some studies show improvements in insulin and metabolic markers, but large reviews found no clear improvement in pregnancy rates compared with placebo.
Bottom line: the 2023 International PCOS Guidelines do not recommend myo-inositol specifically for fertility.
Vitamin D
Low vitamin D is common in PCOS. If you are deficient, supplementation under medical supervision may help metabolic health.
Omega-3 fatty acids
Evidence: May improve triglycerides, insulin markers, and inflammatory markers in PCOS.
N-acetylcysteine (NAC)
May improve insulin resistance, but fertility evidence remains limited.
⚠️ Important note on all supplements
Supplement quality and regulation vary globally. Most are not FDA-regulated. Discuss with your healthcare provider before starting any supplement, especially if you are trying to conceive or undergoing fertility treatment.
Tracking ovulation with PCOS
Irregular cycles make ovulation prediction challenging, but not impossible.
Best methods to track ovulation with PCOS
- Ovulation predictor kits (OPKs): some women with PCOS have elevated baseline LH, which can create false positives. Advanced digital tests that measure both estrogen and LH may be more accurate.
- Basal body temperature (BBT): confirms ovulation after it happens.
- Cervical mucus tracking: offers advance warning of fertility.
Pregmate app + OPKs
The Pregmate app works with Pregmate ovulation tests to help track LH trends and provide personalized cycle predictions, which is helpful for women with irregular PCOS cycles who need to test more often.
When to start testing with irregular PCOS cycles
| Cycle Length | Start Testing (Day) | Expected Positive |
|---|---|---|
| 23-28 days | Day 8-10 | Day 11-14 |
| 29-35 days | Day 12-14 | Day 15-21 |
| 36-42 days | Day 16-18 | Day 22-28 |
| Irregular / very long | Day 10 | Test daily until positive |
Formula: start testing at (shortest cycle length - 17). For very irregular cycles, start early and stay consistent.
Age considerations: best age to get pregnant with PCOS
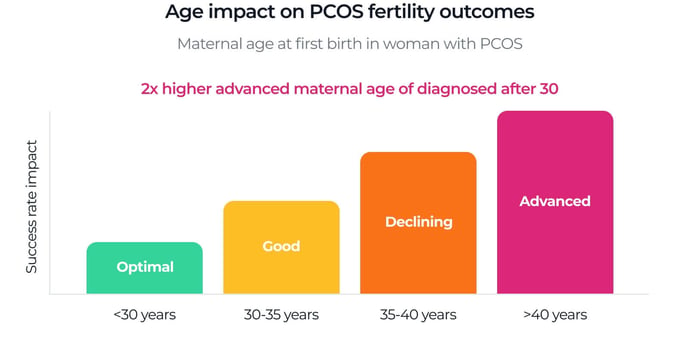
Age is the most critical factor for fertility success, even more so than PCOS status.
- Under 35: highest natural conception and treatment success rates.
- 35-40: success rates decline; earlier fertility evaluation is recommended.
- Over 40: significantly reduced success rates; immediate fertility consultation is recommended.
Key finding from 2024 research
Because PCOS can delay conception, many women with the condition have their first child later in life. This is why tracking your cycle early is so important - it helps you understand your body sooner, so you do not lose valuable time.
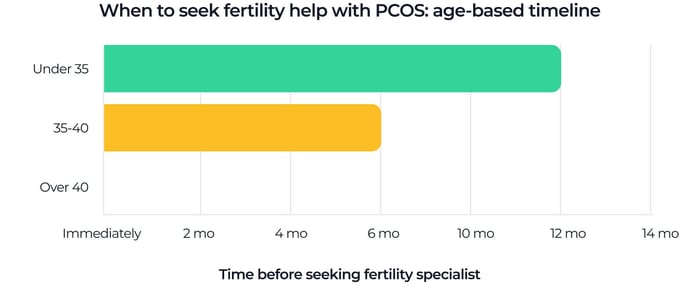
When to seek fertility help with PCOS: age-based timeline
- Under 35: after 12 months of trying.
- Ages 35-40: after 6 months of trying.
- Over 40: immediately.
Pregnancy risks with PCOS: what you should know
A meta-analysis of 104 studies involving 106,690 pregnancies found that women with PCOS have higher odds of pregnancy complications, even when age and BMI are matched:
Pregnancy complication risks: PCOS vs. general population
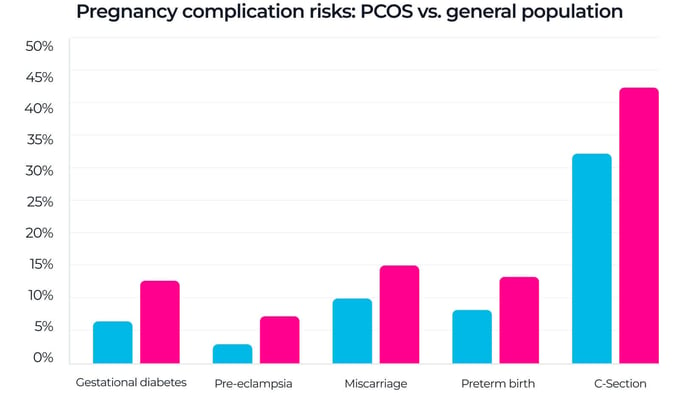
Source: Nature Communications, 2024. "Systematic review and meta-analysis of pregnancy outcomes in women with polycystic ovary syndrome." DOI: 10.1038/s41467-024-49749-1
- Gestational diabetes: increased risk.
- Pre-eclampsia and gestational hypertension: higher odds.
- Miscarriage: elevated risk.
- Preterm birth: higher odds.
- Cesarean section: increased likelihood.
⚠️ Important context
These are increased risks, not certainties. With proper prenatal care and monitoring, many women with PCOS have healthy pregnancies. Early screening and close medical supervision can improve outcomes.
When to see a fertility specialist
Seek evaluation sooner if you have PCOS:
- Under 35: after 6-12 months of trying.
- 35 or older: after 6 months of trying.
- Any age: if you have very irregular cycles or confirmed anovulation.
What to expect
- Hormone testing: LH, FSH, AMH, testosterone, and prolactin.
- Ultrasound: to visualize ovaries and check for cysts.
- HSG test (if needed): to confirm fallopian tubes are open.
- Semen analysis for your partner: to rule out male factor infertility.
Before your first appointment
Bring this info: last 3-6 months of cycle tracking, list of supplements or medications, family history of PCOS or infertility, and your questions.
Ask about: success rates for your age and BMI, treatment timeline, uncovered costs, and what happens if the first treatment does not work.
Remember: you can get a second opinion. If a doctor dismisses your concerns or rushes you, find another one.
Trying to get pregnant with PCOS: realistic expectations
What percentage of women with PCOS get pregnant?
Research indicates that approximately 60-77% of women with PCOS eventually achieve pregnancy, though it may take longer and may require medical assistance in some cases.
Timeline expectations
- Natural conception: may take 12-24 months or longer, depending on ovulation frequency.
- With letrozole: many women conceive within 2-3 treatment cycles.
- With IVF: success varies by age and other factors, but egg numbers may be favorable in PCOS.
The path forward
- Start with lifestyle optimization if overweight.
- Track ovulation to confirm whether you are ovulating.
- Seek medical help early; do not wait a full year automatically.
- Use evidence-based medical treatments like letrozole under physician supervision.
- Be cautious with supplements because current evidence is limited.
Get personalized cycle insights with PCOS
The free Pregmate app helps women with irregular PCOS cycles identify patterns, track LH trends, and get testing reminders based on their unique cycle length.
Frequently asked questions
- Can I get pregnant naturally with PCOS?
- Yes. Many women with PCOS conceive naturally, especially if they ovulate regularly or with lifestyle modifications. Research shows 60-77% of women with PCOS eventually achieve pregnancy, though it may take longer than women without PCOS.
- How long does it take to get pregnant with PCOS?
- What supplements should I take for PCOS fertility?
- Current evidence is not strong enough to recommend most supplements specifically for fertility outcomes. Prenatal vitamins with folic acid are recommended when trying to conceive, and vitamin D should be corrected if deficient.
- Is PCOS pregnancy high-risk?
- Can I track ovulation with PCOS if my cycles are irregular?
- When should I see a fertility specialist for PCOS?
- Seek evaluation earlier than standard recommendations: Under 35 after 6-12 months of trying (vs. standard 12 months), 35 or older after 6 months of trying (vs. standard 6 months), and any age if you have very irregular cycles or confirmed anovulation. Don't wait—early intervention improves outcomes.
- What is the success rate of IVF with PCOS?
It varies significantly. Some women conceive within months, while others may take 1-2 years or longer. With ovulation induction medications like letrozole, many women conceive within 2-3 treatment cycles. Age, BMI, and whether you're ovulating regularly are major factors.
Women with PCOS have higher odds of certain pregnancy complications including gestational diabetes, pre-eclampsia, miscarriage, and preterm birth. However, these are increased risks, not certainties. With proper prenatal care, early screening, and close monitoring, many women with PCOS have healthy pregnancies and babies.
Yes, but it requires more frequent testing. Use ovulation predictor kits (OPKs) starting early in your cycle and test daily (or twice daily). Track cervical mucus and basal body temperature for confirmation. Apps like the Pregmate app can help identify patterns over time, even with irregular cycles.
Women with PCOS may actually have higher IVF success rates than some other infertility diagnoses because they often respond well to ovarian stimulation and produce good numbers of eggs. A 2020 study found women with PCOS had higher pregnancy rates with IVF compared to other infertility causes. However, miscarriage risk is also elevated, so close monitoring is important.
Medical disclainer
This article is for educational purposes only. PCOS requires individualized medical diagnosis and treatment. The information here should not replace professional medical advice.
Important: Treatment responses vary between individuals. Supplement quality and regulation vary globally—most are not FDA-regulated. All medical treatments have potential risks that must be discussed with your healthcare provider.
If you've been trying to conceive for 6-12 months with PCOS (or sooner if over 35), consult a reproductive endocrinologist or OB-GYN.
Pregmate products are ovulation and pregnancy tests for home use. They do not diagnose, treat, or cure any medical condition.
Sources and references
- Forslund et al., 2024. "Fertility and age at childbirth in polycystic ovary syndrome: results from a longitudinal population-based cohort study." American Journal of Obstetrics & Gynecology, November 2024. Fertility and age at childbirth in polycystic ovary syndrome.
- International PCOS Guidelines, 2023-2024. "Systematic review and meta-analysis of pregnancy outcomes in women with polycystic ovary syndrome." Nature Communications, July 2024. Systematic review and meta-analysis of pregnancy outcomes in women with PCOS.
- Bahawi et al., 2023. "Pregnancy Rates in Women With Polycystic Ovary Syndrome Using Letrozole Versus Clomiphene Citrate." Cureus, August 2023. Pregnancy Rates in Women With PCOS Using Letrozole Versus Clomiphene Citrate.
- Dietz de Loos et al., 2023. "Pregnancy Outcomes in Women with PCOS: Follow-Up Study of a Randomized Controlled Three-Component Lifestyle Intervention." Journal of Clinical Medicine, January 2023. Pregnancy Outcomes in Women with PCOS.
- Fitz et al., 2024 "Inositol for Polycystic Ovary Syndrome: A Systematic Review and Meta-analysis to Inform the 2023 Update of the International Evidence-based PCOS Guidelines." Journal of Clinical Endocrinology & Metabolism, May 2024. Inositol for PCOS: systematic review and meta-analysis.
- Frontiers in Endocrinology, 2020. "Pregnancy Outcomes of Women With Polycystic Ovary Syndrome for the First In Vitro Fertilization Treatment." Frontiers in Endocrinology, September 2020. Pregnancy Outcomes of Women With PCOS for the First IVF Treatment.
- Frontiers in Nutrition, 2024. "Efficacy of dietary supplements as an adjunctive therapy for polycystic ovary syndrome: an umbrella meta-analysis." Frontiers in Nutrition, October 2024. Efficacy of dietary supplements as an adjunctive therapy for PCOS.
- SOGC Position Statement, 2025. "Inositol for the Management of Polycystic Ovary Syndrome." Society of Obstetricians and Gynaecologists of Canada, February 2025. SOGC Position Statement


